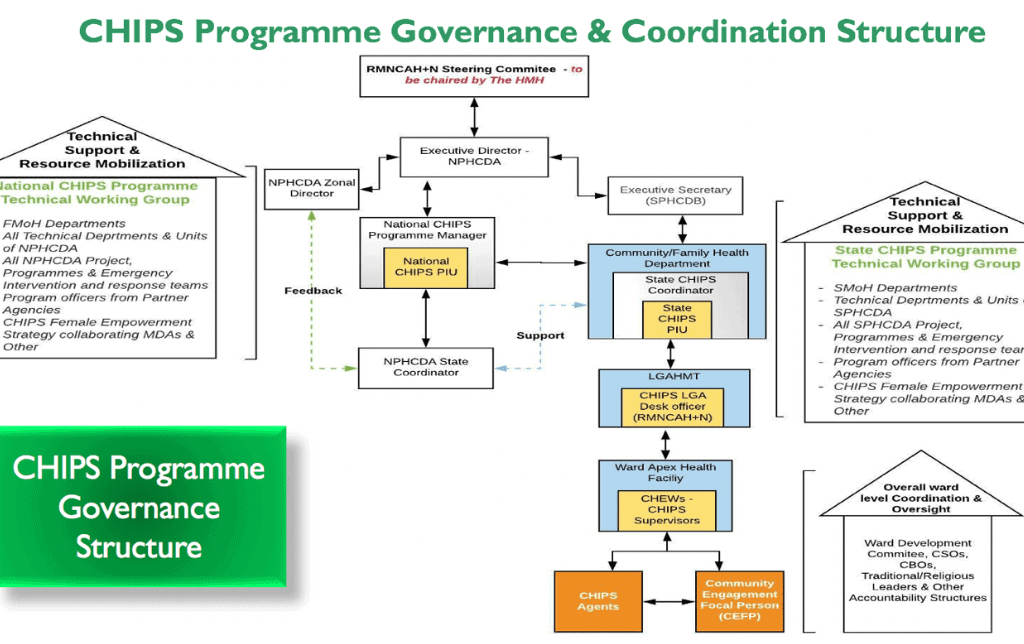
The CHIPS Programme Implementation Unit is made up of six (6) working groups namely;
The CHIPS PIU, led by the Programme Manager, with oversight and support by the ED/CEO of the NPHCDA, coordinates all CHIPS Programme activities at National level, and supports States in the planning and implementation of the CHIPS Programme. This is done in a multi- stakeholder collaborative approach, working with FMOH, other MDAs, Development Partners, Academia, etc.
State CHIPS PIUs, led by the State CHIPS Coordinator, comprises of State Program Officers drawn from relevant thematic areas, with oversight provided by the SPHCDB Executive Secretaries and Directors, drive Programme implementation at the state level, and coordinate, monitor and supervise implementation at lower levels, with support from other MDAs, development/implementing partners, Academia, etc.
An LGA Desk Officer (usually the MCH/RH Officer) is appointed in each implementing LGA to provide daily coordination of the Programme at that level, with oversight from the LGA Health Authority Management Team (LGAHMT).
Ward Development Committees (WDCs), Community-Based Organisations (CBOs), Civil Society Organisations (CSOs), and Traditional and Religious bodies provide the oversight and monitoring of the CHIPS Programme, while daily coordination and direct supervision of CHIPS Personnel is provided by the supervising Community Health Extension Workers (CHEWs) at the ward Focal PHC Facility.
As at October 2021, 19 States across the country are currently in the implementation phase with all State in various stage ranging from State training of Trainers to full deployment of CHIPS Personnel.
The National CHIPS PIU is engaging with other states (17 States and FCT) to commence planning for implementation of the CHIPS Programme. Each state has been assigned state support officers and assisting state support officers to provide technical guidance for the development of an implementation work plan.
Implemented by the FMOH under the Child Health Unit of the Department of Family Health Services, iCCM is a global strategy that seeks to expand access to treatment of leading childhood killer diseases – malaria, pneumonia and diarrhoea in especially hard to reach areas where children under five lack access to health facilities. The strategy uses lay trained community health workers, named CORPS who are trained to diagnose these conditions and provide appropriate therapy.
At the sub-national level, NPHCDA has been working assiduously, with state and non-state actors, to integrate all community based health workers, including CORPs, to ensure the actualization of the CHIPS Programme, in line with the Presidential mandate. To support this process, the Honourable Minister of Health directed the harmonisation of the two programmes, ensuring iCCM is fully integrated into the CHIPS Programme at the National Policy and Strategy level.
The NPHCDA and Department of Family Health at the FMOH have collaborated over the last several months, with other stakeholders from MDAs, Academia, Partners, etc. to operationalise this; the results of which are a set of comprehensive, harmonised CHIPS Documents that will serve as the roadmap for implementation of all community health worker programming in the country. A draft document was developed after a validation workshop held on 25th – 27th October 2021 in Lagos State. This document will be finalised and launched by December 2021.